- Home
- >>
- Summary Notes
- >>
- Basic Science
- >>
- Anatomy
An excellent external resource for anatomy revision: Instant Anatomy – with a book available with the same title.
Gross Structures
Lungs
- Left and Right Lung
- Further Divided into Lobes
- Left Lung has 2 Lobes with an Oblique fissure separating them (also has a pseudo lobe – the lingula (little tongue in latin) most inferiorly
- Right Lung has 3 lobes and two separating fissures:
- The Horizontal fissure separates Upper and Middle lobes. (at the level of the 4th rib)
- The Right Oblique fissure separates Middle and Lower lobes
- All vessels and airways enter the lung via the Hila on each side:


Pleura
The pleura is a large, thin sheet of continuous tissue.
However it is separated into two sections depending on what it surrounds:
- Visceral Pleura – surrounds the lungs
- Parietal Pleura- Surrounds the inside of the chest wall the lungs sit in:
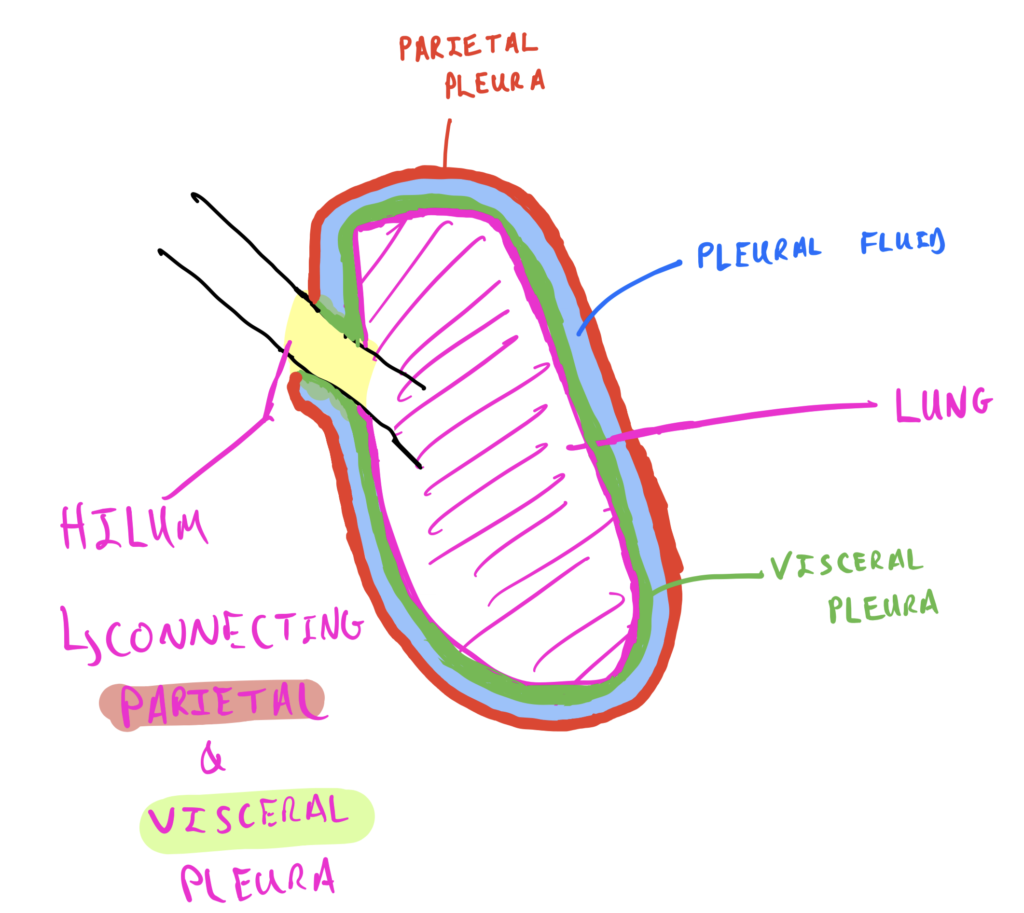
- The entirety of the pleura secretes pleural fluid in the space between the parietal and visceral aspects- The pleural cavity:
- This lubricates the tissue- allowing it to glide over each other.
- Any inflammation in the pleura that stops this smooth gliding can be heard via auscultation – learn more on the Resp Exam Signs page
- The most inferior portion of the pleural cavity is the costodiaphragmatic recess
- The costo-phrenic angle of this is the first area that any excess fluid starts to collect in
- Blunting of this angle suggests excess fluid- this is visible on CXR
Skeletal Structures
- 12 pairs of ribs
- All attach to the spine at 2 points:
- At the junction between the vertebral body of the current rib number and the vertebral body superior to it (IE Rib 2 connected to junction of T2 and T1)
- Exception is rib 1 – only attaches to T1
- Attaches at the tubercle of the spinous process of same rib number
- Both are costo-vertebral joints
- At the junction between the vertebral body of the current rib number and the vertebral body superior to it (IE Rib 2 connected to junction of T2 and T1)
- 10 Attach to the sternum – 2 are “floating” – only attach to the spine
- Made up of: The Manubrium (most superior)
- Connected to the sternal body (via sternal angle)
- Connected to the Xiphoid process (most inferior)
- Ribs attach to sternum via costal cartilage
Muscles of Respiration
Diaphragm
- Innervated by the phrenic nerve
- RAMI OF C3,4 and 5 (C3,4,5 keeps the diaphragm alive)
- Separates the thoracic and abdominal cavity
- Contraction shifts diaphragm inferiorly
- Relaxation shifts diaphragm superiorly
Intercostal Muscles
- 3 layers
- External
- Internal
- Innermost
- Each muscle attaches between two ribs- many muscles in total
- Contract to pull ribs up and out – expanding chest wall and therefore lungs
- Relax to push ribs down and in
Accessory Muscles
To facilitate DEEP inspiration and expiration, utilised in times of stress: additional muscles can be used:
- Deep Inspiration Muscles: – All attach to various ribs to increase speed and rate of chest expansion
- Pectoralis Major
- Pectoralis Minor
- Sternocleidomastoid
- Scalenus Muscles
- Deep Expiration Muscles: – The anterolateral Abdominal Wall Muscles (4 muscle pairs)- contraction results in forcing diaphragm superiorly. -Causes a more forceful expiration.
- Anterior midline muscles- Rectus Abdominus. – “abs”
- Lateral Muscles- 3 layers:
- External Oblique (most superficial)
- Internal Oblique
- Transversus Abdominus
The Respiratory Tract
Facts on each section of the respiratory tract will be given.
The entierty of the respiratory tract (apart from alveoli) are lined with Cilliated Squamous Epithelial
The respiratory tract comprises of:
- Conducting airway -Trachea to the distal bronchioles
- Warm, moisten and clean the air
- Contain Pseudostratified ciliated columnar epithelium with goblet cells throughout. – aka respiratory epithelium.
- Goblet cells produce mucous which lines the walls the air passes through
- Cillia line the walls as well- these are hair-like projections that continuously beat superiorly.
- Combined they form the mucocilliary escalator – cillia work to move trapped material within mucous (dust, bacteria etc) out of the respiratory system.
- Hyaline Cartilage lines the conducting airway (the outside of the tube)
- This provides strength and keeps the airway patent.
- Respiratory Airway -The distal bronchioles and Alveoli
- Participate in gas exchange
There is also an Upper and a Lower Respiratory tract:

Nasal Cavity
- Conchae in LATERAL nasal wall.
- Upper, Middle and Lower
- Space in between each conchae a MEATUS
- Air flows through meatus- warmed (by rich blood supply) and dust/pathogens etc is caught in hairs/mucous in cavity produced by respiratory epithelium
Larynx
- Contains the vocal folds on either side – vibrate for sound- phonation
- Innervated by branches of CNX – Vagus Nerve – any compression(from cancer)/damage results in hoarse voice
- Forms the afferent and efferent limbs of the cough reflex
- When small irritants sensed on vocal folds- signal travels via CNX to brain and output in sequence to:
- Phrenic nerve to diaphragm to stimulate breathing in (pushes diaphragm inferiorly)
- CN X to close vocal cords to start to increase intra-thoracic pressure
- Intercostal nerves to anterolateral abdominal muscles to increase intra-abdominal pressure
- This increase forces diaphragm superiorly
- This increases intra-thoracic pressure
- CNX opens vocal cords
- CNV tenses soft palate to close nasopharynx – so only air goes out of mouth
- Cough occurs
- When small irritants sensed on vocal folds- signal travels via CNX to brain and output in sequence to:
- The space between vocal folds – the rima glottidis
- Air travels through rima glottidis to trachea
- Is the narrowest part of the Upper respiratory tract – after Rima glottidis = Lower resp tract
- Since narrowest- is the point of upper airway obstruction through foreign objects (eg food)
- If the entierty of the rima glottis is obstructed – the cough reflex cannot occur as air cannot enter the lungs to build up in pressure.
- Heimlich manoeuvre aims to overcome obstruction by increasing abdominal pressure to force diaphragm up – increasing overall airway pressure – to dislodge objects from the bottom of resp tract up.
- Since narrowest- is the point of upper airway obstruction through foreign objects (eg food)
- Cartilage of Larynx
Trachea
- Starts at C7 vertebra – directly connects to larynx
- Anterior made up of C-shaped cartilage rings of HYALINE CARTILAGE
- These rings are connected together by fibro-elastic tissue
- Posterior made up of fibro-muscular tissue
Bronchi
- There are 3 levels of bronchi:
- Main bronchi – the 2 largest bifurcating from the trachea at the Carina
- Bifurcation occurs at the level of the T4 Vertebra (in terms of spinal level)/ Sternal angle (in terms of anatomical landmarks)
- Lobar Bronchi – 1 for each lobe
- 2 on left
- 3 on right
- Segmental Bronchi
- 10 on each side
- 20 in total
- Main bronchi – the 2 largest bifurcating from the trachea at the Carina
Bronchioles
Bronchioles have NO Hyaline Cartillage
They instead have smooth muscle which can constrict (broncho-constriction) and relex (broncho-dilation)
- This is influenced by:
- Parasympathetics
- Histamine presence -the basis for allergic asthma triggers (as histamine is released in allergies)
Epithelium within bronchioles goes from : columnar to cuboidal as it goes on
There are 3 sections of bronchioles:
- proper – the majority of the bronchiole
- terminal -the last section to contain NO alveoli
- Contain CLUB CELLS – stem cells that detoxify the environment and modulate the immune system
- respiratory – sections that start to contain alveoli (discontinuously)
Alveoli
Alveoli have extremely thin walls with NO cartillage or smooth muscle
They are mostly (90%) composed of Type 1 Pneumocytes (squamous epithelium) at 1 cell thick – allowing very efficient gas exchange.
Alveoli are lined with alveolar lining fluid (ALF) – This is a water-based solution that allows for more efficient gas exchange between the alveoli and the capillaries surrounding them.
- HOWEVER- due to the surface tension that water-based solutions create (Think of a meniscus with the most superior layer of water being pulled down by other water molecules)
- This would normally cause alveoli to collapse – especially on expiration with a lack of positive air pressure keeping these alveoli patent.
- SURFACTANT is a lipid based solution. – It’s name literally comes from an amalgamation of letters from “anti-surface tension”
- It is made by Type II Pneumocytes – (Polygonal cells) -The other 10% composition of alveoli
- Being lipid-based means it repels the polar water molecules, breaking the surface tension they hold
- This allows alveoli to stay patent with a reduced force causing them to collapse (due to reduced surface tension)
- It is made by Type II Pneumocytes – (Polygonal cells) -The other 10% composition of alveoli
- SURFACTANT is a lipid based solution. – It’s name literally comes from an amalgamation of letters from “anti-surface tension”
Alveoli also contain resident macrophages. These are known as DUST CELLS