- Home
- >>
- Summary Notes
- >>
- Clinical Practice
- >>
- Common Drugs
Antibiotics
Prescribing antibiotics should be a very deliberate action. They should NEVER be misused. Guidelines for antibiotic prescribing are made to be followed as they reduce the chance of antibiotic resistance developing in bacteria.
The concept of antibiotic stewardship is important. This is the continued practice of bettering antibiotic prescribing. This is done through auditing departmental prescriptions to make sure they meet local guidelines. Every locality has different most likely bacteria that cause infections in the area, so guidelines differ from place to place.
The continued rise of resistant strains of bacteria will mean that infections become harder and harder to treat in the future. It is important to counterbalance this with the following tenets of prescribing antibiotics:
- Prescriptions should be:
- The right drug
- At the right time
- At the correct dose
- For the correct duration
Only when a BACTERIAL infection is suspected should antibiotics be prescribed. There should be a very high threshold much of the time for prescribing antibiotics. This is the case especially for UPPER RESP infections as even when bacterial, they are typically self limiting. The majority of these cases are viral.
The first antibiotic prescribed is known as the EMPIRICAL Antibiotic. This covers the most likely organism of infection. It is however important to gain the SENSITIVITY of antibiotic prescriptions (in respiratory medicine this is typically done through a sputum sample or a swab.).
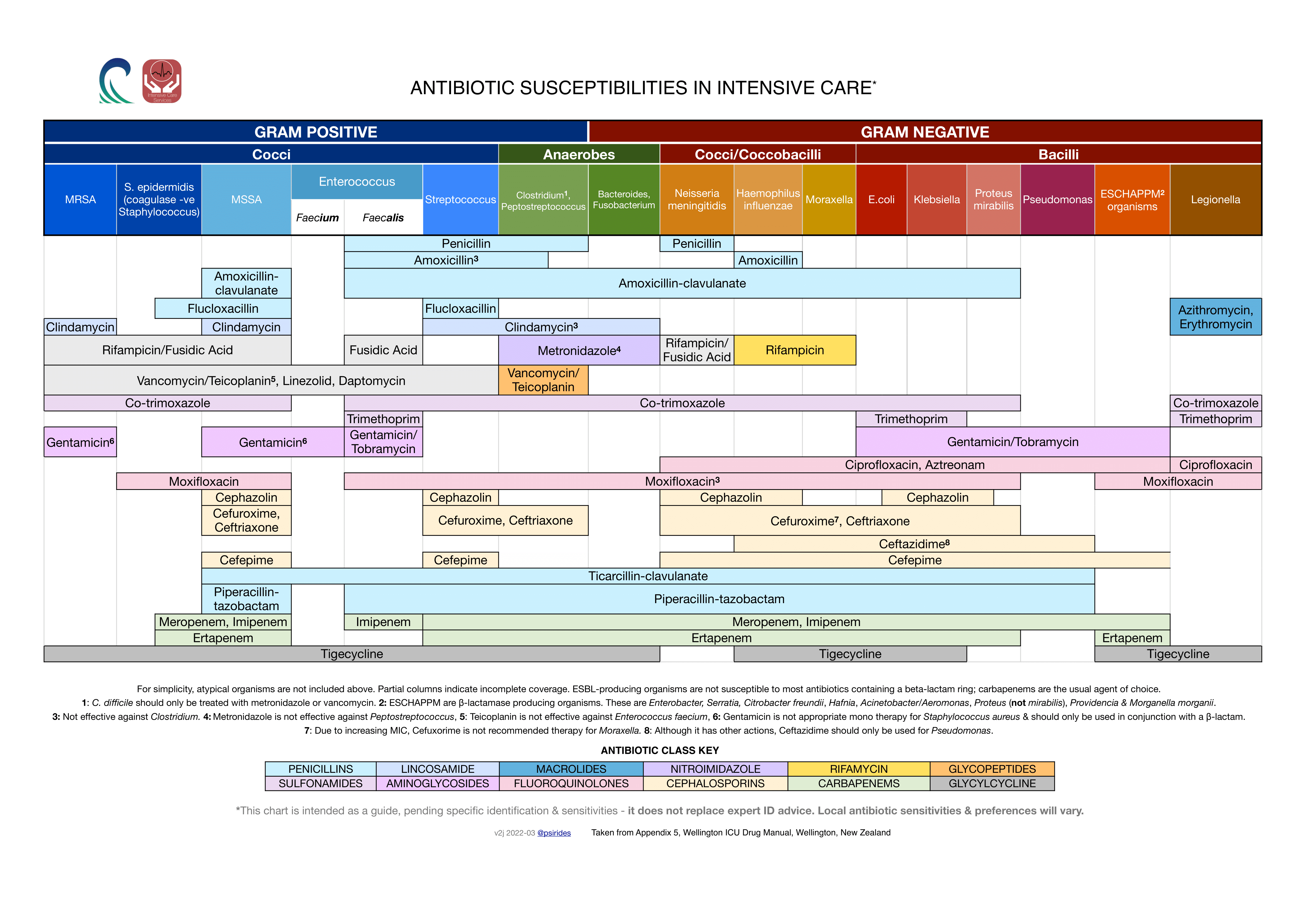
This sensitivity makes sure that the current empirical antibiotic is working. It also allows the possibility of an antibiotic that works on a narrower spectrum to be prescribed- limiting the impact on commensal bacteria (bacteria not causing disease) further limiting the rise of resistance.
The following is a chart of antibiotics and the bacteria they act on to illustrate the concept of ”spectrum of antibiotic action”
Oxygen
Oxygen is a drug. It’s administration should be controlled, as like all drugs, it can have side effects. This is especially true in COPD patients.
Poorly prescribed, oxygen in COPD patients is an oxygen percentage at the wall that is HIGH. This results in the seemingly counter-intuitive result of HYPOXIA and more importantly HYPERCABIA. However when you look at the first principles of physiology the reason becomes clear.
There is a general misconception of this being due to a lack of hypoxic drive and subsequent hypoventilation . Although this may be true for a small minority of patients, the majority will retain carbon dioxide due to V/Q mismatching.
Localised low PaO2 in the lung leads to localised vasoconstriction. This means that with areas of poor ventilation (as happens in COPD due to emphysema) there is no need for good perfusion- as poor gas exchange results in these areas.
Naturally, areas of poor ventilation have appropriately poor perfusion, redirecting blood to areas of better ventilation which in turn allows for optimum gas exchange at areas of lung that have in-tact alveoli. This protects the COPD patient from V/Q mismatch. The following animation illustrates this well:
When oxygen is prescribed inappropriately however at HIGH CONCENTRATIONS. This vasoconstriction does not occur. This leads to inappropriately perfused alveoli that cannot efficiently add O2 OR more importantly REMOVE CO2. The following animation illustrates this:
Inhalers
Inhalers are a drug delivery method unique to respiratory medicine.
The following is a detail of most of the common terms that you can come across with inhalers:
Types of Inhalers
Firstly there are 2 broad types of inhalers:
- Dry powder Inhaler (DPI) –
- These are easier to use, typically given to children/cognitively impaired as it is BREATH ACTUATED.
- Metered Dose Inhaler (MDI) –
- This gives a single puff of drug and so a technique has to be developed to take it properly
- Benefit comes with the wide variety of drugs available
- Also smaller inhaler, so more portable
- Cheaper device
- A SPACER can be attached to MDIs- this has a mask that is attached to a long chamber. This is used for those that struggle with their inhaler technique, and so allows for a complete dose of the drug to be given, as patients can breathe normally. – It is normally used for CHILDREN and the very elderly.
Drug Classes used in Inhalers
SABA/LABA
SAMA/LAMA
ICS
NAMES/colours/brands