- Home
- >>
- Summary Notes
- >>
- Clinical Practice
- >>
- CXR Reading
Introduction
The Chest X-Ray (CXR) is one of the most useful investigations in respiratory medicine.
A solid grounding in CXR interpretation is vital in diagnosing and treating patients.
Much like a history, a systematic approach is the best way to read these (at times) confusing images. It also makes sure you do not miss anything.
There are 3 key things that should be done when looking at any CXR: [D.R.ABCDE]
- Details
- Patient Name, DOB, Date CXR Taken
- RIPENESS (Image Quality)
- ABCDE (systematic assessment)
RIPE
Before analysing an X-ray, its always best to orient yourself and check the quality of the film. – Is the image RIPE?:
Rotation
Are clavicles symmetrical in distance to spine? – Makes sure the image is centred.
Inspiration
Patients hold their breath when images are taken- this is to create as visible a picture as possible.
6 Ribs should be visible if this was done properly – it creates a good image.
If less ribs are visible- can falsely create a pathological looking image:
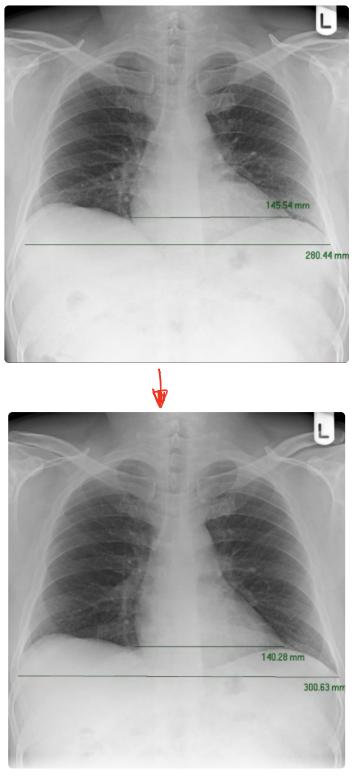
Both images here are well centred.
However in the first image only 4 ribs are visible. – This creates an area at the bottom of the mediastinum that seems consolidated.
This is a poorly inspired film.
The second image is a film from the same patient, however with adequate inspiration, 6 ribs are clearly visible. – Here it is clear that there are no areas of consolidation.
This is a normal CXR.
Picture
What kind of picture are you looking at?
PA view is standard. However AP views are also used in those patients that are unable to stand. lateral views are also used (especially in fracture assessment)
An important point to note about PA and AP views is the apparent different in heart size.
A non-standard AP view can create a picture of false cardiomegaly (enlarged heart):
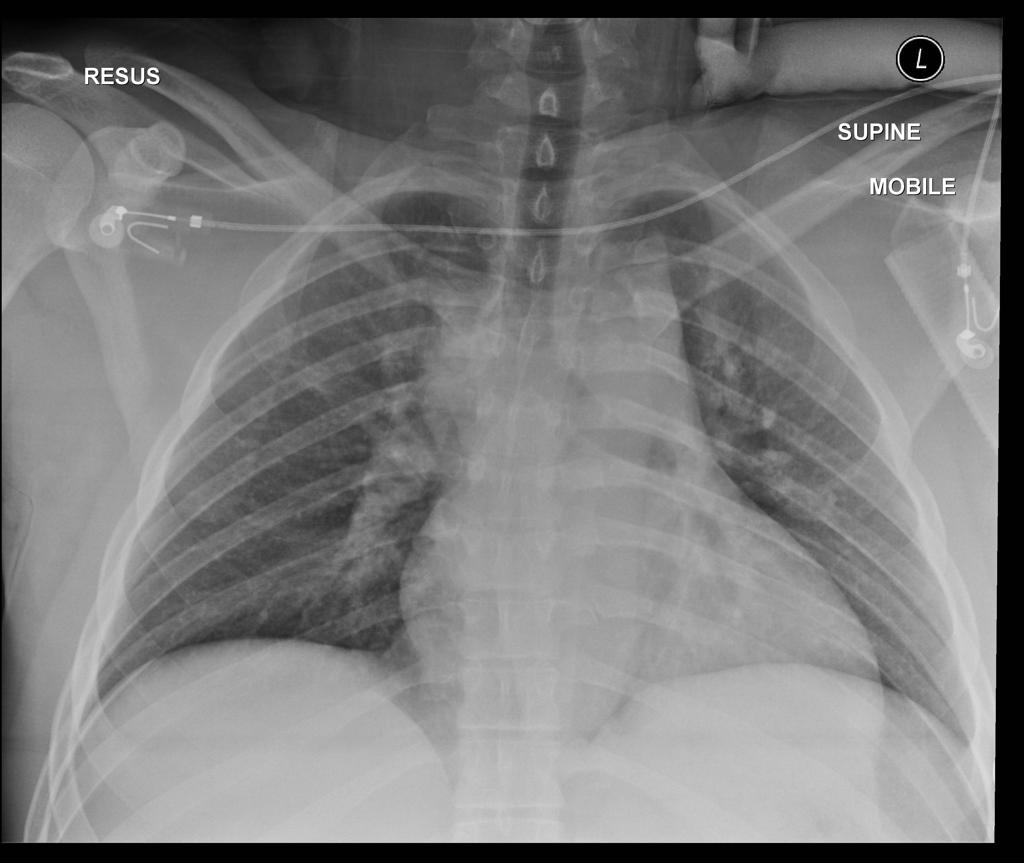
AP view of a CXR shows an enlarged view of the heart.
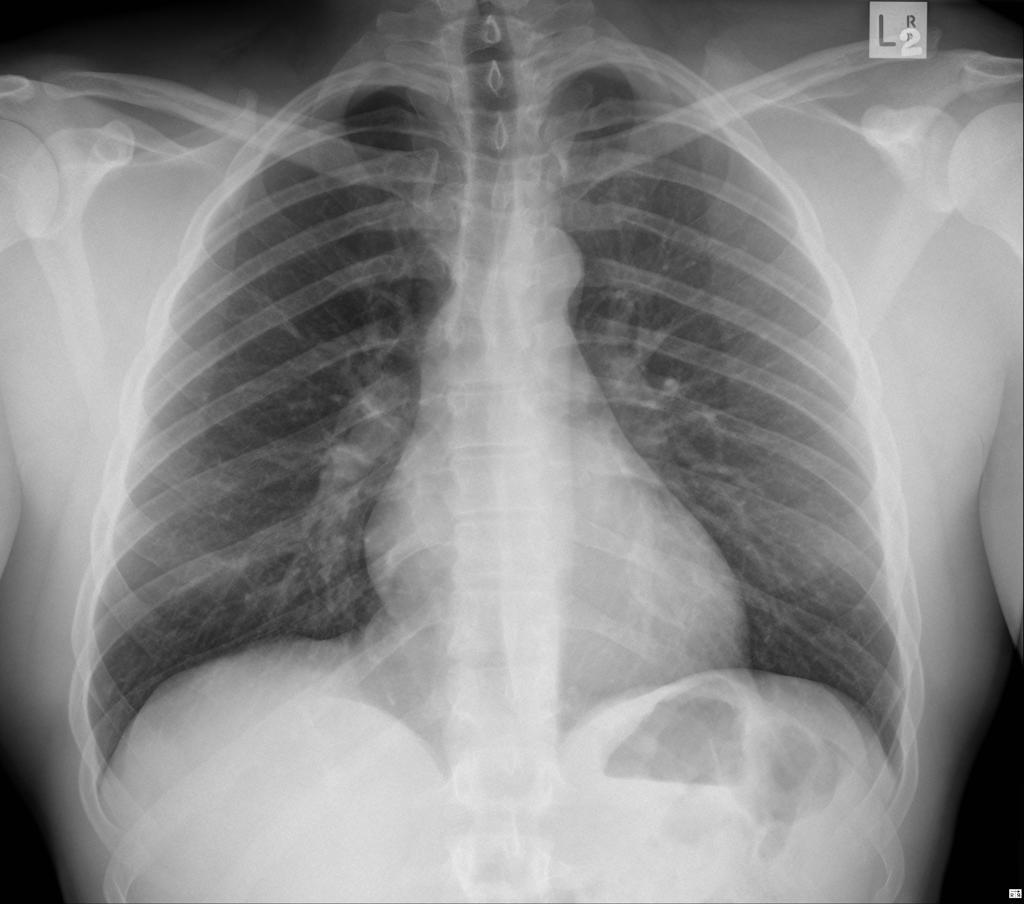
PA view of a CXR from same patient – shows a normal sized heart.
Exposure
Have the X-rays penetrated the heart, allowing you to see behind the heart shadow?
- LEFT hemi-diaphragm visible?
- Spine visible?
ABCDE
The ABCDE acronym is an excellent, memorable approach for CXR analysis and is used by students and consultants alike:
Airway
Think of the big structures leading up to the lungs- assess their position – everything should be central and symmetrical.
Trachea– In a well centred CXR (See RIPE!) this should be right in the middle – any deviation is a massive red flag. -look for masses (think cancer, swollen lymph nodes) and assess for any signs of a pneumothorax or pleural effusion.
Hila– The area where many structure meet and enter the lung. LEFT Hilum sits HIGHER than RIGHT hilum with NO difference in overall size. the following structures are contained within:
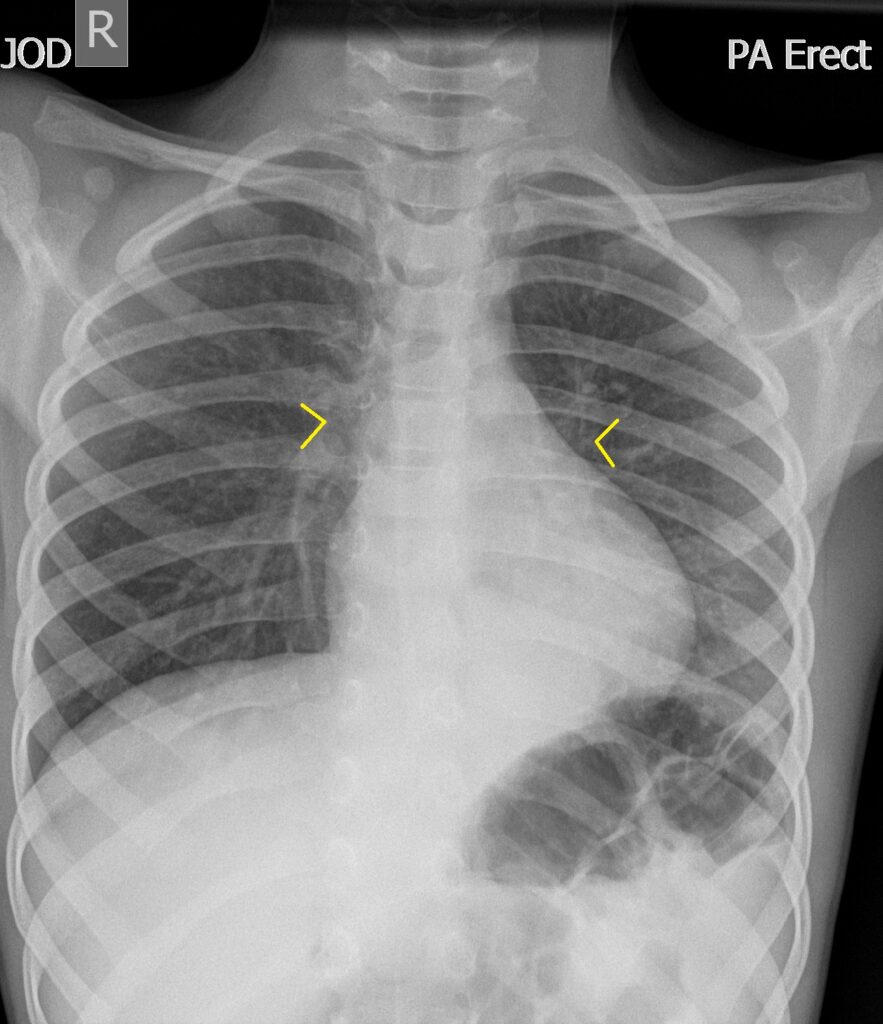
- Pulmonary vasculature
- Forms the overall inward pointing arrow shape (> <) of the hila on each side. – the tip being the hilar point
- Bronchi
- Normally poorly visible unless calcified with age

- Lymph nodes
- If visible and bilateral =sarcoidosis
- If visible and unilateral=
Breathing
Look at the Lungs themselves.
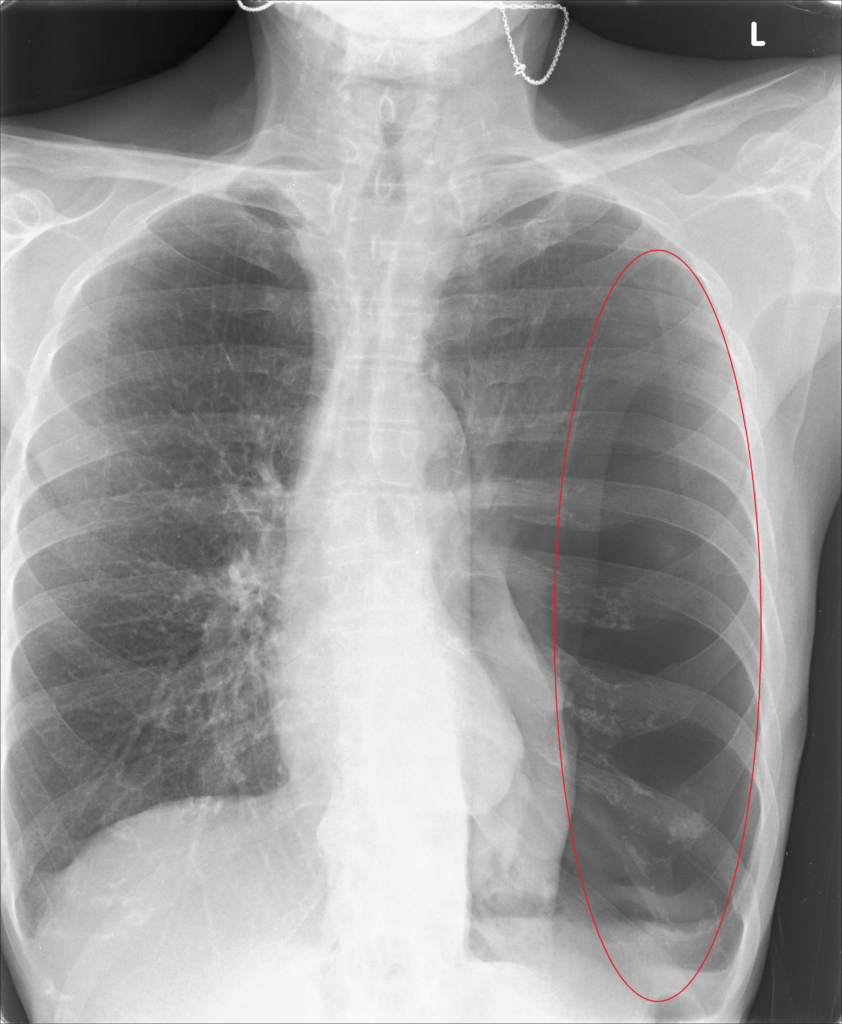
- There should be little lines spreading outwards from the Hila- lung markings.
- Their absence (i.e. pure black space) indicates a pneumothorax.
- On a standard PA film, lung lobes are not visible [they are on a lateral film!]
- The lungs are therefore split into zones – each taking up a third of the height of each lung
- Upper (rib 1-2), Middle (rib 2-4), Lower (rib 4-6)
- Remember they are NOT lobes – the left lung only has 2 lobes but 3 zones – they are just for radiographic description
- This is useful in describing where any pathology is [masses, consolidation]
- The lungs are therefore split into zones – each taking up a third of the height of each lung
- Normally the pleura should NOT be visible. – if seen pleural thickening is evident – indicative of mesothelioma (from asbestosis)
Cardiac
Look at the heart.
As discussed in the RIPE assessment- only a PA view can give a reliable look at the size of the heart.
It should take up a maximum of 1/2 of the width of the chest. If it is more- cardiomegaly is present
A lack of clarity in the borders of the heart indicates specific lobar pathology
- if the RIGHT heart border is not clear- the RIGHT MIDDLE lobe is consolidated
- if the LEFT heart border is not clear- the LINGULA of the LEFT lung is consolidated
Diaphragm and Disability
Look at the area above and below the diaphragm.
The Costophrenic angles above the diaphragm (at the costodiaphragmatic recess) should be sharp and well defined
- Blunting present can be due to a collection of fluid or pus.
The Right hemidiaphragm itself should normally sit higher than the left side (due to the liver pushing it up)
Bubbles of air can exist below the diaphragm. – this is usually normal when it is contained within the stomach.
HOWEVER- if immediately below the diaphragm, it indicates FREE air within the abdominal cavity:
- This indicates bowel perforation – a medical emergency that can quickly lead to sepsis
In terms of disability – it is important to spot any areas of rib fracture. – particularly the LEFT LOWER ribs- as this can lead to splenic rupture – a medical emergency
Everything else
There are often lots of accessory findings including:
- Lines and ECG wires
- NG Tubes
- Artificial heart valves
It is also important to review the edges, the apex and the hila of the lungs once more as abnormality is often missed here.
More Cases
The following is an excellent resource Co-Authored by Dr Tom Fardon and is highly recommended:
Footnote list:
- Case courtesy of Dr Yi-Jin Kuok, Radiopaedia.org. From the case rID: 17910